The Main Roles of the Turbinates
- To direct and maintain laminar airflow, respiratory rate and velocity
- Air Conditioning (Humidification + Heating)
- Filtration
- Olfaction
Directing and Maintainging Laminar Airflow, Respiratory Rate and Velocity
The turbinates project into the nasal cavity, like alongated ridges of erectile mucosal tissues. By doing so, they effectively turn each side of the nasal airway cavity, into a few narrow passages (the “inferior-meatus”, “middle-meatus”, “superior-meatus” and “supreme-meatus”). This way the turbinates are effectively forcing the inspired air to flow in a steady and organized manner, directly to the throat and down to the lungs, and at the same time allow the inspired air to get processed by a maximum amount of nasal tissue, that filters the air, heats it and humidifies it; to keep the airways moisturized, warm and clean, and therefore – open – all the way down to the lungs. Like many other areas in the body – form is function in the nose too. The shape and size, of the structures of the turbinates, allow the nose to function effectively.
|
Fig 15: regular laminar airflow. |
Fig 16: the external cartilaginous nose. |
The turbinates are suspended right in the middle of the inspired nasal airflow current – thus performing two crucial functions: Airflow pattern control and respiratory rate and velocity:
Airflow Pattern Control: The Inferior and middle turbinates act like shutters in an air- conditioner vent – deflecting the airflow in a specific direction and in an orderly manner. This form of stable and orderly airflow pattern is called – Laminar airflow, as opposed to unstable, un-orderly and erratic airflow that is called – Turbulent airflow. Each turbinate encounters the airflow like a wing of a plane – thus splitting the airflow into two currents that curve and stream below and above each turbinate.
Laminar: Oxford English Dictionary – a. consisting of laminae; (Phys., of flow) taking place along fixed streamlines, not turbulent.
Turbulent: Oxford English Dictionary – a. disturbed, in commotion; tumultuous; insubordinate, riotous; (Physic., of flow) having irregular variations in the course of time.
Why is Laminar Airflow so important?
Because when the air flows in a laminar way – it is distributed neatly all over the nasal cavity, under and above the turbinates, reaching the olfactory receptors at the cribriform plate, and ventilating the upper sinuses. In this way the air gets to stream alongside the entire volume of nasal mucosa, with all it’s curves, complicated structures and sinuses – this allows the inspired air to receive maximum levels of heat and humidity from the turbinates and the rest of the nose. This heat and especially – humidity – are crucial for pulmonary health and function, and any reduction in it will cause breathing difficulties, fatigue, and long term nasal and perhaps even pulmonary complications (nasal – atrophic rhinitis, chronic sinusitis, pulmonary – asthma, chronic obstructive pulmonary disease – COPD, etc`).
|
Fig 17 (a): Laminar distribution of airflow. |
Fig 17 (b): Front (anterior) head of right infeior-turbinate. |

The shape of the anterior head of the inferior turbinate makes sure that the majority of inspired air, which has to be used for breathing, is directed to flow through the middle meatus (the space between the inferior and middle turbinates). A smaller portion streams along the inferior meatus, and a tiny portion (not more than 10% of the inspired air) will reach the olfactory bulbs, carrying odorants (scent molecules).
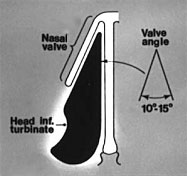
Fig 18: Front (anterior) head of right infeior-turbinate.
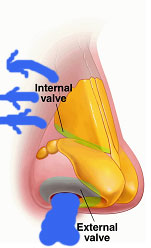
The inspired airflow gets sucked in through the anterior nares, and reaches the narrowest point of nasal airway – the nasal valve (see Figure19). The nasal valve is the main focal point as far as how the optimal nasal resistance and the optimal airflow pattern and velocity in the nose are achieved. It is also where the airflow turns from vertical to horizontal. It can be described as the place where the front (anterior) head of the inferior turbinate and lateral wall, the septum, and the airway’s floor, meet to direct and deflect the majority of airflow coming through the nasal valve to the nasopharynx, to flow through the middle meatus (the open space remaining between the inferior and the middle turbinates).
Importance of Laminar Air-flow in Maintaining Respiratory Rate and Velocity:
Respiratory Rate & Velocity: It is safe to conclude that if any of the turbinates are resected, especially the inferior turbinates, which are the largest ones and occupy all the lower and widest chamber of the nasal cavities (where most of the air flows through), then the airflow pattern changes dramatically, from a steady organized current, known as “laminar” airflow, into a much more erratic and unstable current, known as “turbulent” airflow.
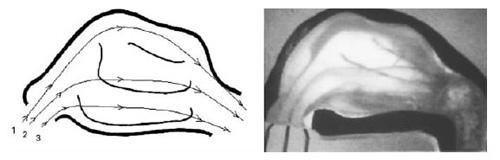
Fig 19: Internal valve (scheme)
This turbulent airflow causes many problems:
a) Shortness of breath: Although a larger amount of air can now enter the nose at once, the air scatters all over the nose, as there are no inferior turbinates to direct it towards the throat. This means that the lungs have to work harder to force the air to stream in an ordered and steady way through the nose towards the trachea. This manifests itself as a form of nasal obstruction called “paradoxical obstruction” – the paradox being, that although the nose is now more open, it is actually harder to force the air straight to the back of the nose and down the throat to the trachea because of the now too wide nasal cavity that although allows a larger intake of air it also allows it to disperse all over the place instead of forcing it to stream along the inferior meatus. Thus, it becomes much harder for the lungs to suck in enough air, especially during any activity, and the result is – chronic shortness of breath, known as dyspnea. This is perhaps the main interference that an ENS patient feels. This disturbance exists even when an ENS patient lies down to sleep. This happen because in a supine position it is much harder for a person to breath in than in an upright position. A human being needs to be able to breath in fast and deep, to over come the natural narrowing of the airways, while lying down. This effective breathing is supported by the healthy nose that provides humidified, warm and filtered air, fast enough to keep the soft-tissue airways of the lungs as open, as moisturized and as clean as possible – to allow the inspired air to reach the lungs as soon as possible, and in optimal conditions for the lungs to operate in.
b) Loss of nasal sensations (including some of the ability to smell): A healthy nose senses the inspired airflow. It has nerve receptors that sense the pressure of the airflow, and different points along the nose, and the temperature of the air. These receptors send feedback to the brain as to whether the airflow is progressing smoothly through the nose, and whether it’s temperature is warm enough. If, for example the brain gets a message that there is too much obstruction it fires back an order that causes the turbinates to decongest (shrink) and allow, more air to pass through, or if it senses that the air is too cold – it will order the turbinates to congest (expand) so that the air will have to pass over a larger amount of turbinate tissue, and therefore will heat up more. A healthy nose also smells well. When the airflow becomes too turbulent, the ability of the nose to sense the air – diminishes greatly. Now the air doesn’t flow smoothly over the motion and temperature receptors, and the air molecules don’t rise high enough, to reach the higher regions of the nasal cavity where the smell receptors are located.
This phenomenon of “Paradoxical Obstruction” has been demonstrated in many experiments. Here are some pictures from a recent study:
“The combination of acoustic rhinometry, rhinoresistometry, and flow simulation in noses before and after turbinate surgery: a model study”, Grutzenmache S., Lang C., Mlynski G., ORL, 2003 (65),: 341 – 347:
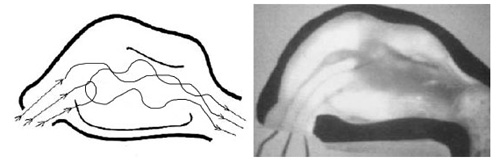
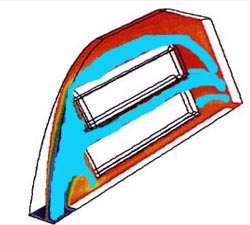
Fig 20: Flow pattern in Normal nose. 1=Ventral part of the inspiration stream, 2=Central part of the stream, 3=Dorsal part of the stream.

Fig 22: Flow pattern in nose after inferior turbinectomy.
Through comparing these pictures to each other– one can easily see that only in the normal nose (Fig 20) does the airflow spread evenly in a laminar tidy fashion and flow alongside all three nasal structures of turbinates.
Looking at Fig-21 (post middle turbinectomy) reveals that the airflow converges all into the middle meatus, and hardly passes through the inferior meatus or supreme meatus (where the olfactory receptors are).
Looking at Fig-22 (post inferior turbinectomy) reveals that the entire airflow converges to flow along the nasal floor. The picture shows clearly – that hardly any air reaches above the middle meatus (which is effectively non-existent now because of the removal of it’s lower component – the Infeior Turbinates), not to mention the superior and supreme areas.